Childbirth is one of the most important moments of women in life, moreover, childbirth is also a challenging moment for women because they need to make a big effort in order to have a successful delivery, and the delivery process always brings serious physical and psychological problems for women after childbirth whether the pain of delivery was hard or slight. We called the key term “birth traumas”.
The following multi-causal and multi-dimensional problems after childbirth often might be ignored by women themselves and their family. But in fact, it always leave negative effect on women’s health. When I was working as a physiotherapist in China, I found that most of female patients have big or small health problems after parturition and some problems are serious which we called pelvic floor dysfunction(PFD): chronic pain of pregnancy, urinary incontinence and postpartum depression and so on. There are many researches noting that pregnancy and childbirth are risks factors concerning postpartum problems. However, when I talked these problems with female patients, especially about delicate health issues, female patients are very embarrassed and they are reluctant to say it out, hiding true feelings and viewing it as normal phenomenon, they prefer suffering from these problems for their whole lifetime instead of seeking for help. Sometimes, female patients hold the view that they can not share their problems with physio of same sex since patients have humiliation. Meanwhile, my male colleagues talked to me that they also have difficulties when communicating with patients of the opposite sex about obscure problems because mutual incomprehension. Hence, it makes hard when I attempt to collect information from my female patients about childbirth diseases.
Recently I left for United Kingdom to study and receive further education. When I communicated with my tutor and classmates who have different culture backgrounds about the development of postpartum rehabilitation in their country and ask them how they consider these issues relating to women’s health, I still felt some of them do not want to discuss with me about the question in depth due to privacy even though they know women’s health should be taken into consideration. In recent years, postpartum rehabilitation is under the development in China because there is a growing realization that these problems could not be completely cured without clinical interventions. Also, in the long run , these problem will become very serious which lead to poor quality of health for women.
In this blog, my aim is to discuss three main problems of puerpera, assessment of disease and existing treatment from the recent research. As I have mentioned before, according to several communications with people of different cultures, I believe that these problems affect every culture and need to be concerned and welcomed, we should encourage women to speak out their real feeling and receive postpartum rehabilitation treatment. I will explain my views from my clinical experiences and evidence-based information. If you would like to make a contribution to my opinions and efforts in mummy’s health, just sharing your views and/or previous experiences, you are more than welcome.
In the last blog, I will discuss about a common mental health disease after childbirth :postpartum depression(PPD) which always affects life of women, children and their family. Some studies found a higher occurrence rate of gastrointestinal symptoms or infant diarrhea among children if their mothers have depressive symptoms (Darcy et al., 2011, Rahman et al., 2004). Another reason for concern is that the risk of negative-infant feeding would be increased and reduce the time of breast feeding because of depressed mothers. As time goes by, their babies would have more frequent hospital visits and emergency room visits(Brummelte S et al., 2016). As a result, if postpartum depression is not being taken seriously, it will lead to serious impact on mummy and their children. As I mention before, delivering a baby is the challenge, but it is also an emotional rush like no other. A research suggested that there are 3 types of postpartum dysphoric mood states: the maternity blues (a fairly common, transient disorder), postpartum affective psychosis (relatively rare), and postpartum depression (as many as 20% of postpartum women may cause mild depression)(Hopkins et al., 1984). Therefore, only postpartum depression need to be concerned and have enough studies for the moment.
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), 6 has defined this perspective by introducing the term“with postpartum onset”to distinguish major depressions that after 4 weeks when a mummy deliver a baby(depression et al., 2004). Beck highlighted that about 13% of women suffer from postpartum depression and because the symptom is secret that made it is difficult to early recognize this disease, and the result showed that there are four new indicators of postpartum depression:self-esteem, marital status, socioeconomic status, and unplanned/unwanted pregnancy(Beck et al., 2001). In general, many of risks is included into scales and these instruments could identify some female who have risk of postpartum depression and become the base that healthcare provider could communicate with pregnant sufferers. However, these instruments might over identify some women at risk or miss some women who experience postpartum depression.
Postpartum depression always about women’s psychological factors, in clinical practice, clinical doctors need to use an acceptable,convenient standardized screening instrument such as the Edinburgh Postnatal Depression Scale(EPDS) when they face their female patients. From Harris B’s paper, Edinburgh Postnatal Depression Scale(EPDS) has been confirmed to have specificity of 93% and a sensitivity of 95%(Harris B et al., 1989). In low-risk population screening studies, Appleby found that with the use of the Edinburgh Postnatal Depression Scale, the rates of postpartum depression(Edinburgh Postnatal Depression Scale score >10) ranged from 14% to 21% (Appleby et al., 1997), and patients with great awareness of depressive symptoms may be more likely to seeking for professional help.
Then my aim is to explore existing treatment for postpartum depression, Perfetti J highlighted that mummy’s chronic postpartum depression is associated with delay in language learning and the developement of cognition as well as behavioral difficulties when children go to the school at first. Therefore,this makes it very important that a female with postpartum depression shoud be treated in an appropriate way in order to decrease damage upon children and avoid recurrence of depression symptoms. On the one hand, research illustrated that several types of psychotherapy that could be recommend to be effective way: individual interpersonal psychotherapy, cognitive behavioral therapy, and group or family therapy(Clark R et al., 2003). In addition, the family-focused group model consider mother-infant and family relationship which could be more comprehensive way to relieve depressive symptoms as well as reducing social isolation(Perfetti J et al., 2004).
On the other hand,psychotropic medication is the other existing way for postpartum depression. However, this is concern whether psychotropic medication have potential effects for pregnant women and children. The recommended practice is conducting an individualized and careful risk-benefit analysis for each female patients whether psychotropic medication is suitable for them. So it is important to assess the impact of prescribing antidepressant medication for every patient who has postpartum depression. From Antonuccio DO’s research, it showed that psychotherapy is equally effective to medication in the clinical practice(Perfetti J et al., 2004). Moreover, Poyatos‐León’s research found that physical exercise during pregnancy and after childbirth is a safe way to achieve better psychological well-being and to reduce postpartum depression symptoms (Poyatos‐León et al., 2017). Therefore, if we integrate well with the psychotherapy and physical exercise, female patients would receive good treatment result.
From my experience, there does not have systematic independent clinics provide services for women who have postpartum depression, the reason is that we do not have professional special physiotherapist for postpartum depression at the moment. Therefore, it makes the outcome of clinical treatment is less than satisfactory. Overall, a trend is the rehabilitation medicine service in which something is developing over time, postpartum rehabilitation system would be more specialized. Hence, the development of childbirth care could be positive for the well-being of women, their infants and families.
Thank you very much for reading my blog, I am enjoying to writing about postpartum rehabilitation of my interests, meanwhile, I hope you could enjoy reading my blog. If you have any question, please feel free to leave your comments.
REFERENCE:
Bagley, Anita & Foti, Theresa; Davids, Jon R.; Bagley, Anita, 2000. Abiomechanical analysis of gait during pregnancy. Journal of Bone and Joint Surgery, 82(5), pp.625–32.
Shi-Qiong Li et al., 2017. Effect of pelvic floor rehabilitation technique in preventing the postpartum pelvic floor dysfunction. Journal of Hainan Medical University, 23(4), pp.129–132.
Opala-Berdzik, A. et al., 2010. The Influence of Pregnancy on the Location of the Center of Gravity in Standing Position. Journal of Human Kinetics, 26(1), pp.5–11.
Vermani, E., Mittal, R., & Weeks, A. (2010). Pelvic girdle pain and low back pain in pregnancy: a review. Pain Practice, 10(1), 60-71.
Sabino, J., & Grauer, J. N. (2008). Pregnancy and low back pain. Current reviews in musculoskeletal medicine, 1(2), 137-141.
Stapleton DB, MacLennan AH, Kristiansson P. The prevalence of recalled low back pain during and after pregnancy: a South Australian population survey. Aust N Z J Obstet Gynaecol. 2002;42(5):482–485. doi:10.1111/j.0004-8666.2002.00482.x
Albert, H., Godskesen, M., & Westergaard, J. (2001). Prognosis in four syndromes of pregnancy‐related pelvic pain. Acta obstetricia et gynecologica Scandinavica, 80(6), 505-510.
Mørkved, S., & Bø, K. (2014). Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinence: a systematic review. Br J Sports Med, 48(4), 299-310.
Mogren, I. M. (2006). BMI, pain and hyper-mobility are determinants of long-term outcome for women with low back pain and pelvic pain during pregnancy. European spine journal, 15(7), 1093-1102.
Franke H, Franke JD, Belz S, Fryer G. Osteopathic manipulative treatment for low back and pelvic girdle pain during and after pregnancy: A systematic review and meta-analysis. J Bodyw Mov Ther. 2017;21(4):752–762. doi:10.1016/j.jbmt.2017.05.014.
Licciardone, J. C., Stoll, S. T., Fulda, K. G., Russo, D. P., Siu, J., Winn, W., & Swift Jr, J. (2003). Osteopathic manipulative treatment for chronic low back pain: a randomized controlled trial. Spine, 28(13), 1355-1362.
Elden, H., Ladfors, L., Olsen, M. F., Ostgaard, H. C., & Hagberg, H. (2005). Effects of acupuncture and stabilising exercises as adjunct to standard treatment in pregnant women with pelvic girdle pain: randomised single blind controlled trial. Bmj, 330(7494), 761.
Nilsson‐Wikmar, L., Pilo, C., Pahlbäck, M., & Harms‐Ringdahl, K. (2003). Perceived pain and self‐estimated activity limitations in women with back pain post‐partum. Physiotherapy Research International, 8(1), 23-35.
Huskisson EC. Measurement of pain. Lancet 1974; 2:1127–1131.
Milsom I, Altman D, Lapitan MC, et al. Epidemiology of urinary (UI) and faecal incontinence(FI) and pelvic organ prolapse (POP). In: Abrams P, Cardozo L, Khoury S,Wein A. Incontinence 4th International Consultation on Incontinence. Committee 1.Birmingham, UK:Health Publication Ltd, 2009:35–111.
Dumoulin, C., Hay‐Smith, J., Habée‐Séguin, G. M., & Mercier, J. (2015). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women: a short version Cochrane systematic review with meta‐analysis. Neurourology and urodynamics, 34(4), 300-308.
Swift, S. E. (2000). The distribution of pelvic organ support in a population of female subjects seen for routine gynecologic health care. American journal of obstetrics and gynecology, 183(2), 277-285.
DeLancey JO, Kearney R, Chou Q, et al. The appearance of levator ani muscle abnormalities in magnetic resonance images after vaginal delivery. Obstet Gynecol2003;101:46–53.
Lee, H. N., Lee, S. Y., Lee, Y. S., Han, J. Y., Choo, M. S., & Lee, K. S. (2013). Pelvic floor muscle training using an extracorporeal biofeedback device for female stress urinary incontinence. International urogynecology journal, 24(5), 831-838.
Yun JM, Kim SJ, Lee KS (2000). The effect of pelvic floor muscle training with biofeedback and functional electrical stimulation for genuine stress urinary incontinence. Korean J Urol 41:627–632.
O’Sullivan, P. B., Caneiro, J. P., O’Keeffe, M., Smith, A., Dankaerts, W., Fersum, K., & O’Sullivan, K. (2018). Cognitive functional therapy: an integrated behavioral approach for the targeted management of disabling low back pain. Physical therapy, 98(5), 408-423.
Depression, C. P. (2004). Can postpartum depression be predicted?. Primary Psychiatry, 11(3), 42-47.
Beck, C. T. (2001). Predictors of postpartum depression: an update. Nursing research, 50(5), 275-285.
Appleby, L., Warner, R., Whitton, A., & Faragher, B. (1997). A controlled study of fluoxetine and cognitive-behavioural counselling in the treatment of postnatal depression. Bmj, 314(7085), 932.
Mogren, I. M. (2007). Does caesarean section negatively influence the post-partum prognosis of low back pain and pelvic pain during pregnancy?. European Spine Journal, 16(1), 115-121.
Almeida, E. C. S., Nogueira, A. A., Candido dos Reis, F. J., & Rosa e Silva, J. C. (2002). Cesarean section as a cause of chronic pelvic pain. International Journal of Gynecology & Obstetrics, 79(2), 101-104.
Wijma, J., Potters, A. E. W., Tinga, D. J., & Aarnoudse, J. G. (2008). The diagnostic strength of the 24-h pad test for self-reported symptoms of urinary incontinence in pregnancy and after childbirth. International Urogynecology Journal, 19(4), 525-530.
Mens, J. M., Damen, L., Snijders, C. J., & Stam, H. J. (2006). The mechanical effect of a pelvic belt in patients with pregnancy-related pelvic pain. Clinical biomechanics, 21(2), 122-127.
Bertotto, A., Schvartzman, R., Uchôa, S., & Wender, M. C. O. (2017). Effect of electromyographic biofeedback as an add‐on to pelvic floor muscle exercises on neuromuscular outcomes and quality of life in postmenopausal women with stress urinary incontinence: A randomized controlled trial. Neurourology and urodynamics, 36(8), 2142-2147.
Hopkins, J., Marcus, M., & Campbell, S. B. (1984). Postpartum depression: a critical review. Psychological bulletin, 95(3), 498.
Brummelte S, Galea LA. Postpartum depression: Etiology, treatment and consequences for maternal care. Horm Behav. 2016;77:153–166. doi:10.1016/j.yhbeh.2015.08.008.
Perfetti J, Clark R, Fillmore CM. Postpartum depression: identification, screening, and treatment. WMJ. 2004;103(6):56–63.
Darcy, J. M., Grzywacz, J. G., Stephens, R. L., Leng, I., Clinch, C. R., & Arcury, T. A. (2011). Maternal depressive symptomatology: 16-month follow-up of infant and maternal health-related quality of life. J Am Board Fam Med, 24(3), 249-257.
Harris, B., Huckle, P., Thomas, R., Johns, S., & Fung, H. (1989). The use of rating scales to identify post-natal depression. The British Journal of Psychiatry, 154(6), 813-817.
Clark, R., Tluczek, A., & Wenzel, A. (2003). Psychotherapy for postpartum depression: a preliminary report. American Journal of Orthopsychiatry, 73(4), 441-454.
Poyatos‐León, R., García‐Hermoso, A., Sanabria‐Martínez, G., Álvarez‐Bueno, C., Cavero‐Redondo, I., & Martínez‐Vizcaíno, V. (2017). Effects of exercise‐based interventions on postpartum depression: A meta‐analysis of randomized controlled trials. Birth, 44(3), 200-208.
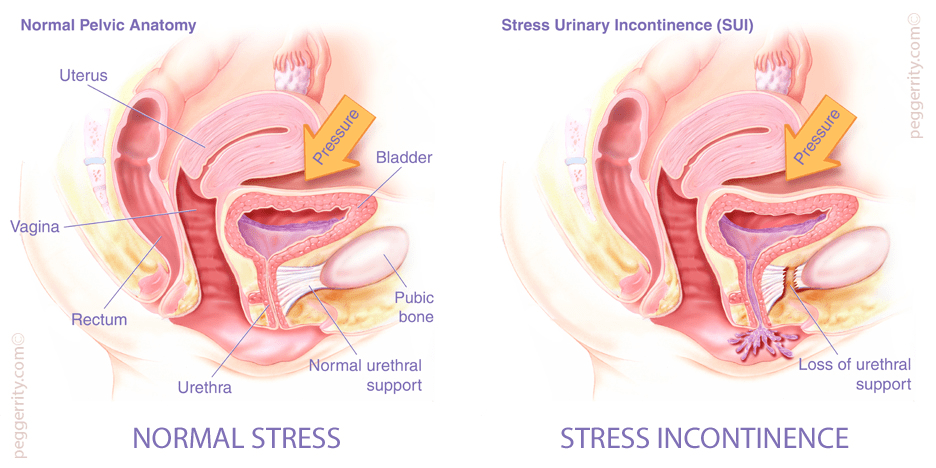
In this blog, I am going to touch on one other of most common problems during pregnancy and after childbirth:Urinary incontinence(UI), evaluation and possible interventions. Urinary incontinence(UI) is a prevalent symptom of pelvic floor dysfunction(PFD) and leads to poor quality of life and withdrawal from fitness and exercise activities. Urinary incontinence (UI) is defined by the International Continence Society as the complaint of any involuntary loss of urine. It is demonstrated that urinary incontinence is divided into three forms: urge urinary incontinence (bladder dysfunction)(UUI), stress urinary incontinence (sphincter dysfunction)(SUI), and mixed urinary incontinence (both sphincter and bladder dysfunction)(MUI). Dumoulin highlighted that isolated stress urinary incontinence (SUI) accounts for half of all urinary incontinence(UI), with most studies reporting 10% to 39% prevalence. During pregnancy, the pelvic floor muscle is relaxed because of continuous pressure and when a mummy deliver a birth, it could be stressful for the pelvic floor structure and pelvic muscle, and still existing after childbirth (Dumoulin et al., 2015). As a research claimed that, pregnancy and childbirth are considered as risk factors for making the perineum and pelvic floor muscles weaken and injured. And because pregnancy and delivery lead to damage and stretch of pelvic floor muscle fibers type I and II, then it always develop into stress urinary incontinence. From Mørkved’s research, a sequence of stretch and rupture of peripheral nerves and connective tissue and muscles cause urinary incontinence problem(Mørkved et al., 2014). Swift’s research highlighted that a half of women suffer from pelvic floor function dysfunction due to childbirth (Swift et al., 2000). With ultrasound and MRI, injuries of pelvic floor muscles is about 20-26% following vaginal childbirth(DeLancey et al., 2003). Therefore, these evidence confirmed that vaginal delivery can be regarded as equal to a major sport injury.
Unfortunately, there exists conception that urinary incontinence(UI) is a secret problem that most female do not have the courage to seek for professional consultation, so urinary incontinence(UI) has not been given attention concerning prevention or treatment. In my opinion, the earlier pregnant sufferers pay attention to urinary incontinence(UI) and consult professional physiotherapist, the better result they can get after suitable treatment. In the next part, I will take some time to tell you existing treatment for urinary incontinence(UI) and improve the awareness of this condition’s treatability!
When the physio give a full diagnosis of urinary incontinence for their patients, they always ask patient’s medical history, give physical examination, urinalysis and assess the quality of life, existing interventions can include non-surgical options(such as lifestyle modifications, pelvic floor muscle training and drugs) to improve the capacity of pelvic floor muscle and bladder. As for future directions in research may focus on environmental and genetic factors for urinary incontinence(UI).
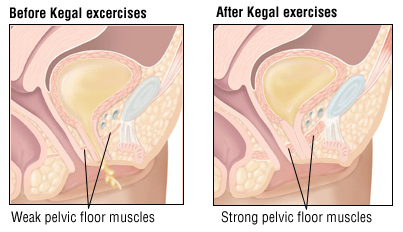
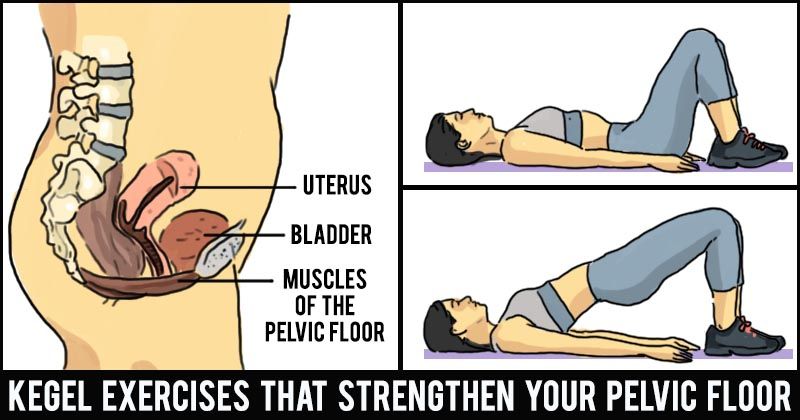
The goal of treatment is to improve the capacity of anal contraction and do postpartum exercise with physiotherapist’s guidance. But most mummy actually do not know how to use pelvic floor muscles accurately, therefore, that results in low exercise efficiency, which would induce a treatment that called pelvic floor muscles training programmes(PFMT). Pelvic floor muscles training(PFMT) has been a part of training programmes in Chinese Taoism for over 6000 years (Chang et al., 1984). Morris highlighted in a research that illustrated rest and tension of pelvic floor muscles which introduced pelvic floor muscles training(PFMT) as a prevention and treatment option for urinary incontinence(UI) to the British physiotherapy profession(Morris et al., 1936). Furthermore,from Dumoulin’s research, pelvic floor muscles training(PFMT) is the commonly used physical therapy especially for puerpera who have stress urinary incontinence(SUI)(Dumoulin et al., 2015). However, pelvic floor muscles training(PFMT) as a treatment for stress urinary incontinence(SUI) did not become popular until after the mid-1900s when American gynaecologist Arnold Kegel reported on the successful treatment of 64 cases of female SUI using pelvic floor muscle exercises with a pressure biofeedback perineometer (Kegel et al., 1948). More recently, pelvic floor muscles training(PFMT) was defined by an international standardization committee as an exercise to improve pelvic floor muscle strength, endurance, power, relaxation or a combination of these parameters (Bø et al., 2017). A research showed that pelvic floor muscles training(PFMT) had successful outcome rates varying from 21 % to 84 %, although it has been found to have better subjective than objective outcomes(Yun JM et al., 2000). As for time to training pelvic floor muscles, if it is earlier to be trained, it might be less likely to have severe pelvic floor dysfunction(PFD), for example, urinary incontinence. Moreover, even if it is injured, training pelvic floor muscles could improve pelvic floor dysfunction(PFD) as it has already know how to use pelvic floor muscles accurately and maintain exercise. Some researches demonstrate that spontaneous delivery can cause abnormal pelvic floor mechanism in the early stage, and enhance the occurrence rate of pelvic floor dysfunction(PFD), which can severely affect the women’s health and life quality. Currently, it is generally believed that early pelvic floor muscle training after delivery has a certain effect in preventing pelvic floor dysfunction(PFD) in the gestational period and after delivery. According to current exercise guidelines, it encourages all pregnant women to keep active during weekdays during pregnancy and after childbirth including cardiovascular and strength training exercise(Mørkved, S et al., 2014). From Bertotto’s research, it shows that there is Pelvic floor muscle training using extracorporeal biofeedback(BF) can be an effective and safe conservative treatment option for female stress urinary incontinence(SUI) without the discomfort caused by vaginal sensors. With the addition of biofeedback(BF), female patients could produce the neuroplasticity or functional neural regeneration mechanisms of the central nervous system, in this case, they could have ability of controlling and monitoring pelvic floor muscle motor pattern and when the activity is happened, they would know how to cooperate with their physiotherapist(Bertotto et al., 2017).
Some researches demonstrated that the second labor stage extension, multiple production, and perineal laceration can damage the pelvic floor, we could understand how important it is for a woman to do specific pelvic floor exercises. Moreover, pelvic floor muscles training(PFMT) also applies for everyone, especially for most elder women that they could come across urinary incontinence in their subsequent lives, so they also need to know pelvic floor muscles training(PFMT) which would be beneficial for their daily lives. Recently, Kegel principles is part of the pelvic floor muscles training(PFMT) in the clinical practice, so with well-timed exercise which include Kegel or pelvic floor muscle exercises, it is supposed to increase muscle strength and reduce urinary incontinence frequency. Furthermore, Mørkved illustrated a recommended training pattern following strength-training principles which lasts at least 8 weeks (Mørkved et al., 2014).
From Wijma’s research, in clinical practice, when pregnant women receive pelvic floor muscles training(PFMT) and trained for quiet a while, physio could give an evaluation to confirm whether problem could be alleviated, that is 20-minute padtest in which 10 jumping jacks were substituted for the standard jumping exercises,and a digital examination(Wijma et al., 2008). In my opinion, with the help of quantitative evaluation of result, physio and female patients could have a direct view on progress of treatment and use pelvic floor muscles training(PFMT)accurately. Current guidelines for exercise during pregnancy shows it lack of adequate evidence for female who have urinary incontinence(UI) problems, so in the near future, I will do more systematic research on the treatment of urinary incontinence(UI).
In my experience, there were lots of independent clinics and they always combine with confinement center in China, they provide a series of treatment for women who have urinary incontinence problems. However, some of clinics do not give an evaluation for every pregnant sufferers and lack of specific rehabilitation plan. Therefore, patients may not receive expectant results and even pose a threat to mummy’s health and their babies. This is because the clinics do not have professional physio and perfect rehabilitation system to guide the whole rehabilitation process. In conclusion, i recommend that pregnant sufferers consult their physio at first and then seek for professional help to decrease damage.
In my next section, I will discuss the last main problem:postpartum depression during and after pregnancy, if you feel interested and have enough patience, please go with my next blog.
In the first blog, I want to talk about physical pain of pregnancy, evaluation and a form of treatment. For most female, when we ask about the pain during pregnancy or postpartum, they described symptoms that pain distribute in low back, lumbar and pelvic region(Sabino et al., 2008). In the recent research, the pain could be summed up in two aspects: pregnancy-related pelvic girdle pain (PGP) and pregnancy-related low back pain (PLBP). In reality, these conditions are very common in puerpera and also can be the reason for sick leave(Mens et al., 2006). Hence, the pregnancy-related pelvic girdle pain(PGP) and pregnancy-related low back pain(PLBP) would influence daily life of women. Research revealed that in the period of pregnancy, lumbal pain is almost stable while the sense of pelvic pain may increase. Moreover, one-third of pregnancy women suffer from severe problem(Mogren et al., 2007). After delivering baby, the morbidity of low back and pelvic pain(LBPP) is from 5% to 40% in half a year, even after 3 years, about 20% of women with back pain symptoms have consistent symptoms and postpartum pain is also associated with movement-related activities. Furthermore, postpartum back problems have been found not to be a unitary concept. From Vermani ’s research, the universality of pregnancy-related pelvic girdle pain(PGP) and/or pregnancy-related low back pain(PLBP) is around 45% of all pregnant women and 25% of all postpartum women (Vermani et al., 2010). In consideration of different childbirth ways, it does not have enough evidence to support whether caesarean section (CS) affects the symptoms of low back and pelvic pain or not. However, Almeida stated that caesarean section (CS) is the reason of low back pain and pelvic joint pain( Almeida et al., 2002), but this view also need more evidence to support it and update in the near further.
However, pain of pregnancy is often considered by obstetricians as a common phenomenon and regarded as normal condition for post-birth female. They told female patients that there not a particularly effective measure to cope with the common pain problems. Therefore, most of women do not have the desire to consult and seek for help. As research revealed that the treatment for pain of pregnancy is self-management or prescribed by health professionals is unclear, so the existing perspective is that pregnancy-related pelvic girdle pain (PGP) and pregnancy-related low back pain (PLBP) is an expected part after delivery and there is no treatments being offered and available in clinical institutions for most females(Stapleton et al., 2002). As Albert’s research showed in the survery of 314 female patients, around 8.5% women after childbirth still suffer severe pain in the pelvic joint after two years(Albert et al., 2001). As a consequence, like I mention before, pain problems can not relieved automatically without any clinical intervention.
When considering about factors that may result in pregnancy-related pelvic girdle pain (PGP) and pregnancy-related low back pain (PLBP), a research illustrated that body mass index(BMI) and hypermobility are dominant determinants of persistent body pain, the outcome of research showed that increased body weight and hypermobility lead to strain on the joints, ligaments and muscles, therefore , it may impede or delay remission of low back pain and pelvic pain(LBPP) after pregnancy(Mogren et al., 2006). When a women become a mummy, the uterus gradually stretched and the body weight gravity axis changed because of infant birth weight and gestation duration (Shi-Qiong Li et al., 2017). From the research of Foti, during the gestation process, women have changes in the hormonal and biomechanical aspects and reflect in their weight, weight distribution, joint laxity, musculotendinous strength (Foti et al., 2000). There is evidence in the literature that women put on weight in pregnancy is between 9kg and 14 kg and this weight gain is mainly located in the trunk and the lower trunk, in most cases, the body weight increase 0.29kg every week(Opala-Berdzik et al., 2010). Therefore, the abdominal pressure can produce strong pressure on the pelvic floor muscles and trunk region, that always bring a series of pain problems.
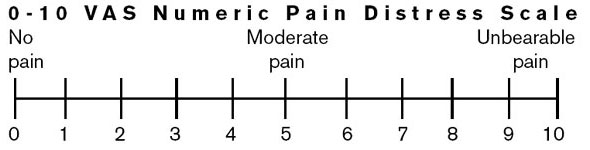
According to Franke et al’s study, osteopathic manipulative treatment (OMT) could bring benefits for pregnant or postpartum women with low back pain(LBP), but result of research may not work in the future, and high-quality randomized controlled trials with robust comparison groups are recommended(Franke et al., 2017). From the Licciardone’s study, it suggested us the osteopathic manipulative treatment(OMT) lasts 15 to 30 minutes, and the techniques consisted a combination of the following manual techniques: myofascial release, strain-counterstrain, muscle energy, soft tissue, high-velocity-low-amplitude thrusts, and cranial-sacral. The osteopathic manipulative treatment(OMT) is a health approach which was aim at physical dysfunction in the low back or adjacent areas. And before applying into practice, practitioners need to evaluate patient’s medical history and physical examination. According to Nilsson-Wikmar’s research, pain could be evaluated with a visual analogue scale(VAS,0-100 mm), and zero as “no pain” , 100 was defined as”the worst imaginable pain”, so when patients described the area of pain and the type of pain sensation to physio, they could mark on a pain drawing(Nilsson-Wikmar et al., 2003). On the one hand, the osteopathic manipulative treatment(OMT) provided by osteopathic manipulative medicine specialist. But more studies with more experienced osteopathic manipulative treatment(OMT) providers and better control of interventions are needed to determine whether osteopathic manipulative treatment(OMT) is beneficial manipulation technique when treat with female patients or whether they may because of placebo effects(Licciardone et al., 2003). On the other hand, stabilising exercises also recommended for pelvic girdle pain during pregnancy, the training started by emphasising activation and control of local deep lumbopelvic muscles, then for the next session, it is designed with dynamic exercise which is focused on more superficial muscles in order to improve mobility, strength, and endurance capacity of low back and pelvic girdle. Also, the outcome of this research illustrated that stabilising exercises would be effective complements to standard treatment for pregnant women with pelvic girdle pain(Elden et al., 2005).
Example of a VAS
Furthermore, a research showed that for disabling low back pain(LBP) patients, cognitive functional therapy was developed as a comprehensive approach that is related to individual’s feeling about pain, social circumstances and body lifestyle factors and so on. And this new approach is not only a basic rehabilitation therapy, in fact, it integrated with behavioral psychology and neuroscience(O’Sullivan et al., 2018). As far as I am concerned, pregnancy-related low back pain belongs to low back pain, so in the course of clinical treatment, professional physiotherapist should consider mummy’s psychological factors, family aspects and body lifestyle factors as well. As a result, physiotherapist could receive a more complete evaluation before treatment and give a systematic treatment plans for patients.
Overall, I personally believed that before choosing existing treatment options, pregnant patients should consult a professional physio and have a comprehensive evaluation of body, though there are also needed more robust evidence to support treatment when give a rehabilitation plan for pregnant sufferers, it should not be ignored the importance of considering suitable intervention for relieving pain of pregnancy and continuous negative effects, and if being taken seriously by obstetricians and attach great importance to this issue, the confirmation of existing treatment techniques and exploration of more effective measurements are likely to happen.
Thank you very much for reading my first blog talking about chronic pain syndromes, and I would do more research on this problem in my next learning process. In my next blog, I will talk about urinary incontinence for puerpera. If you enjoyed this article, please leave a comment and read more!