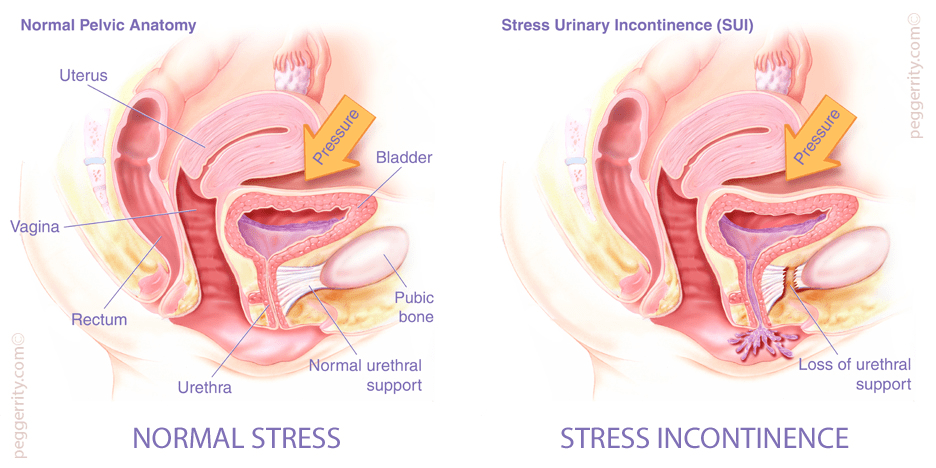
In this blog, I am going to touch on one other of most common problems during pregnancy and after childbirth:Urinary incontinence(UI), evaluation and possible interventions. Urinary incontinence(UI) is a prevalent symptom of pelvic floor dysfunction(PFD) and leads to poor quality of life and withdrawal from fitness and exercise activities. Urinary incontinence (UI) is defined by the International Continence Society as the complaint of any involuntary loss of urine. It is demonstrated that urinary incontinence is divided into three forms: urge urinary incontinence (bladder dysfunction)(UUI), stress urinary incontinence (sphincter dysfunction)(SUI), and mixed urinary incontinence (both sphincter and bladder dysfunction)(MUI). Dumoulin highlighted that isolated stress urinary incontinence (SUI) accounts for half of all urinary incontinence(UI), with most studies reporting 10% to 39% prevalence. During pregnancy, the pelvic floor muscle is relaxed because of continuous pressure and when a mummy deliver a birth, it could be stressful for the pelvic floor structure and pelvic muscle, and still existing after childbirth (Dumoulin et al., 2015). As a research claimed that, pregnancy and childbirth are considered as risk factors for making the perineum and pelvic floor muscles weaken and injured. And because pregnancy and delivery lead to damage and stretch of pelvic floor muscle fibers type I and II, then it always develop into stress urinary incontinence. From Mørkved’s research, a sequence of stretch and rupture of peripheral nerves and connective tissue and muscles cause urinary incontinence problem(Mørkved et al., 2014). Swift’s research highlighted that a half of women suffer from pelvic floor function dysfunction due to childbirth (Swift et al., 2000). With ultrasound and MRI, injuries of pelvic floor muscles is about 20-26% following vaginal childbirth(DeLancey et al., 2003). Therefore, these evidence confirmed that vaginal delivery can be regarded as equal to a major sport injury.
Unfortunately, there exists conception that urinary incontinence(UI) is a secret problem that most female do not have the courage to seek for professional consultation, so urinary incontinence(UI) has not been given attention concerning prevention or treatment. In my opinion, the earlier pregnant sufferers pay attention to urinary incontinence(UI) and consult professional physiotherapist, the better result they can get after suitable treatment. In the next part, I will take some time to tell you existing treatment for urinary incontinence(UI) and improve the awareness of this condition’s treatability!
When the physio give a full diagnosis of urinary incontinence for their patients, they always ask patient’s medical history, give physical examination, urinalysis and assess the quality of life, existing interventions can include non-surgical options(such as lifestyle modifications, pelvic floor muscle training and drugs) to improve the capacity of pelvic floor muscle and bladder. As for future directions in research may focus on environmental and genetic factors for urinary incontinence(UI).
https://www.health.harvard.edu/a_to_z/urinary-incontinence-a-to-z
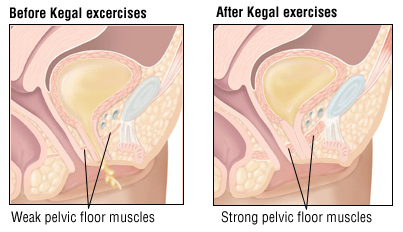
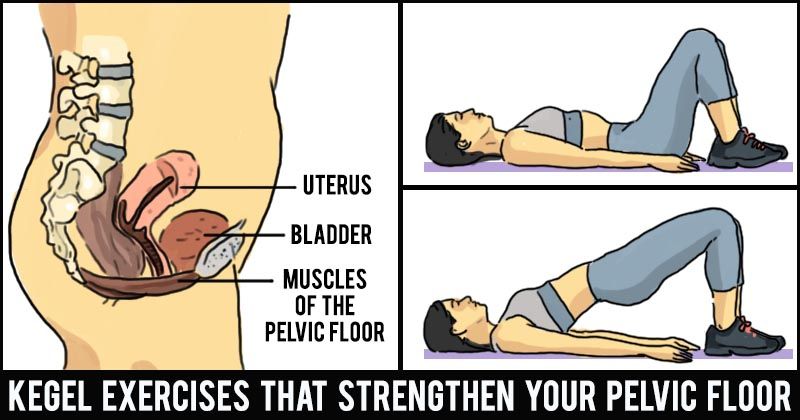
The goal of treatment is to improve the capacity of anal contraction and do postpartum exercise with physiotherapist’s guidance. But most mummy actually do not know how to use pelvic floor muscles accurately, therefore, that results in low exercise efficiency, which would induce a treatment that called pelvic floor muscles training programmes(PFMT). Pelvic floor muscles training(PFMT) has been a part of training programmes in Chinese Taoism for over 6000 years (Chang et al., 1984). Morris highlighted in a research that illustrated rest and tension of pelvic floor muscles which introduced pelvic floor muscles training(PFMT) as a prevention and treatment option for urinary incontinence(UI) to the British physiotherapy profession(Morris et al., 1936). Furthermore,from Dumoulin’s research, pelvic floor muscles training(PFMT) is the commonly used physical therapy especially for puerpera who have stress urinary incontinence(SUI)(Dumoulin et al., 2015). However, pelvic floor muscles training(PFMT) as a treatment for stress urinary incontinence(SUI) did not become popular until after the mid-1900s when American gynaecologist Arnold Kegel reported on the successful treatment of 64 cases of female SUI using pelvic floor muscle exercises with a pressure biofeedback perineometer (Kegel et al., 1948). More recently, pelvic floor muscles training(PFMT) was defined by an international standardization committee as an exercise to improve pelvic floor muscle strength, endurance, power, relaxation or a combination of these parameters (Bø et al., 2017). A research showed that pelvic floor muscles training(PFMT) had successful outcome rates varying from 21 % to 84 %, although it has been found to have better subjective than objective outcomes(Yun JM et al., 2000). As for time to training pelvic floor muscles, if it is earlier to be trained, it might be less likely to have severe pelvic floor dysfunction(PFD), for example, urinary incontinence. Moreover, even if it is injured, training pelvic floor muscles could improve pelvic floor dysfunction(PFD) as it has already know how to use pelvic floor muscles accurately and maintain exercise. Some researches demonstrate that spontaneous delivery can cause abnormal pelvic floor mechanism in the early stage, and enhance the occurrence rate of pelvic floor dysfunction(PFD), which can severely affect the women’s health and life quality. Currently, it is generally believed that early pelvic floor muscle training after delivery has a certain effect in preventing pelvic floor dysfunction(PFD) in the gestational period and after delivery. According to current exercise guidelines, it encourages all pregnant women to keep active during weekdays during pregnancy and after childbirth including cardiovascular and strength training exercise(Mørkved, S et al., 2014). From Bertotto’s research, it shows that there is Pelvic floor muscle training using extracorporeal biofeedback(BF) can be an effective and safe conservative treatment option for female stress urinary incontinence(SUI) without the discomfort caused by vaginal sensors. With the addition of biofeedback(BF), female patients could produce the neuroplasticity or functional neural regeneration mechanisms of the central nervous system, in this case, they could have ability of controlling and monitoring pelvic floor muscle motor pattern and when the activity is happened, they would know how to cooperate with their physiotherapist(Bertotto et al., 2017).
Some researches demonstrated that the second labor stage extension, multiple production, and perineal laceration can damage the pelvic floor, we could understand how important it is for a woman to do specific pelvic floor exercises. Moreover, pelvic floor muscles training(PFMT) also applies for everyone, especially for most elder women that they could come across urinary incontinence in their subsequent lives, so they also need to know pelvic floor muscles training(PFMT) which would be beneficial for their daily lives. Recently, Kegel principles is part of the pelvic floor muscles training(PFMT) in the clinical practice, so with well-timed exercise which include Kegel or pelvic floor muscle exercises, it is supposed to increase muscle strength and reduce urinary incontinence frequency. Furthermore, Mørkved illustrated a recommended training pattern following strength-training principles which lasts at least 8 weeks (Mørkved et al., 2014).
From Wijma’s research, in clinical practice, when pregnant women receive pelvic floor muscles training(PFMT) and trained for quiet a while, physio could give an evaluation to confirm whether problem could be alleviated, that is 20-minute padtest in which 10 jumping jacks were substituted for the standard jumping exercises,and a digital examination(Wijma et al., 2008). In my opinion, with the help of quantitative evaluation of result, physio and female patients could have a direct view on progress of treatment and use pelvic floor muscles training(PFMT)accurately. Current guidelines for exercise during pregnancy shows it lack of adequate evidence for female who have urinary incontinence(UI) problems, so in the near future, I will do more systematic research on the treatment of urinary incontinence(UI).
In my experience, there were lots of independent clinics and they always combine with confinement center in China, they provide a series of treatment for women who have urinary incontinence problems. However, some of clinics do not give an evaluation for every pregnant sufferers and lack of specific rehabilitation plan. Therefore, patients may not receive expectant results and even pose a threat to mummy’s health and their babies. This is because the clinics do not have professional physio and perfect rehabilitation system to guide the whole rehabilitation process. In conclusion, i recommend that pregnant sufferers consult their physio at first and then seek for professional help to decrease damage.
In my next section, I will discuss the last main problem:postpartum depression during and after pregnancy, if you feel interested and have enough patience, please go with my next blog.

2 replies on “let us deal with Urinary Incontinence!”
Hi Helen! Nice blog!
Do you think all women should be offered post-partum physiotherapy?
赞赞
hello, i think women who deliver their baby always need postpartum rehabilitation, but for urinary incontinence, most women would have this problems in the near future, so it should not be ignored.
赞赞